Livedo reticularis related to physical activity: A case report
Livedo reticularis is a skin finding consisting of transient or persistent, macular, violaceous, connecting rings that form a netlike cyanotic pattern. This appearence may be caused by any situation which is related to increase of visibility of the venous plexus under the dermal layer. Thinning of the dermis in elderly people is one of the causes of this lesion without any pathology. Venodilation (triggered by hypoxia or autonomic dysfunction) and blood deoxygenation (ie. venous thrombosis, vasospasm or increased blood viscosity) are two major causes of venous plexus visibility. Although, in most cases livedo reticularis is a result of a physiological response to cold exposure, it can also be a cutaneous sign of an underlying disease such as antiphospholipid syndrome or Sneddon’s syndrome. In this paper, we present a 40 year old female patient having cutaneous manifestations exacerbated by physical activity and who got primary livedo reticularis diagnosis after the exclusion of any underlying pathologies and relation to temperature as in the case of physiological livedo reticularis. Albeit exercise is recommended for the treatment of livedo reticularis because increased circulation helps to dilate the blood vessels throughout the body it is contraversial as in this case exercise was what exacerbated the situation.
Full Article
Introduction
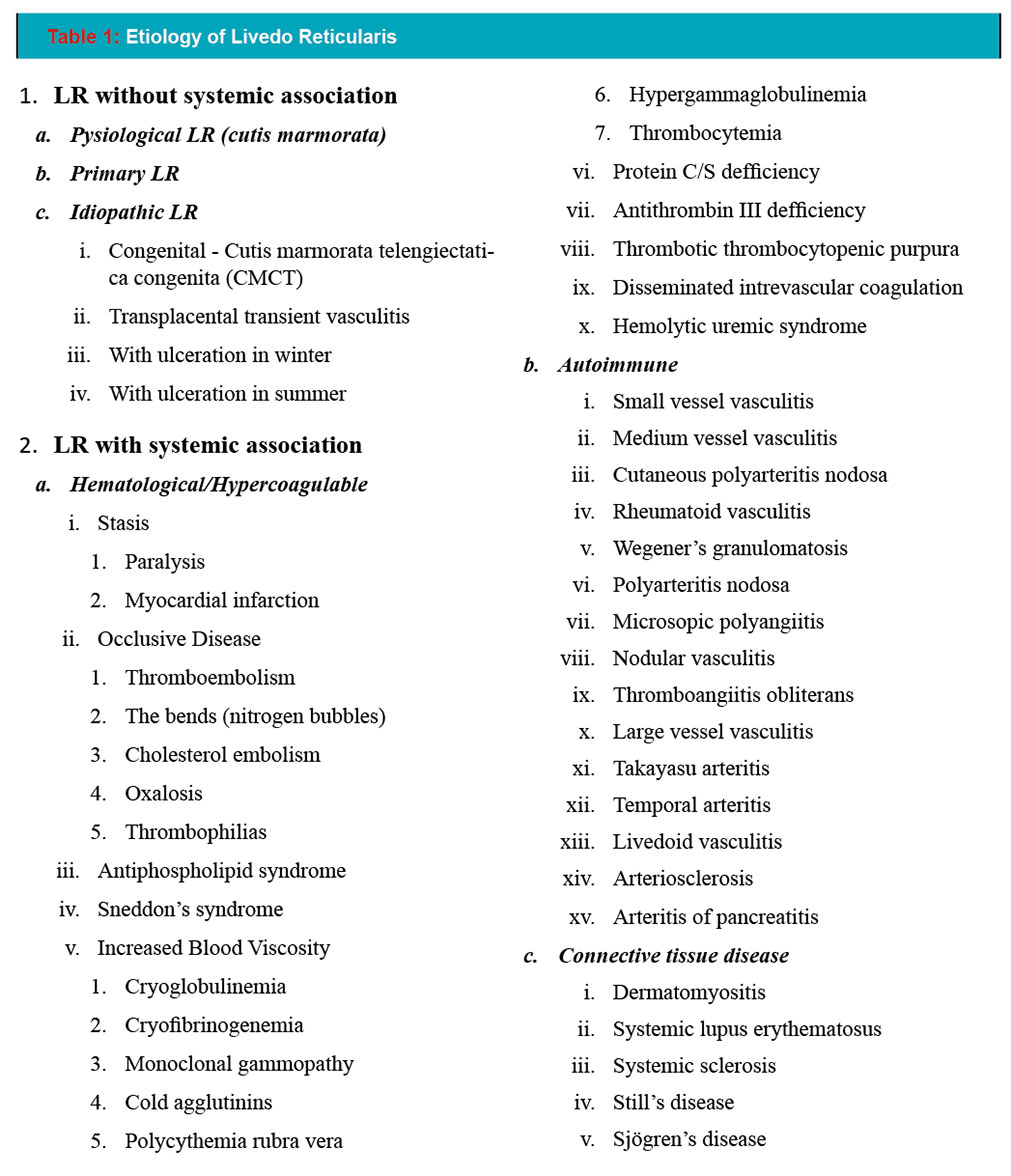
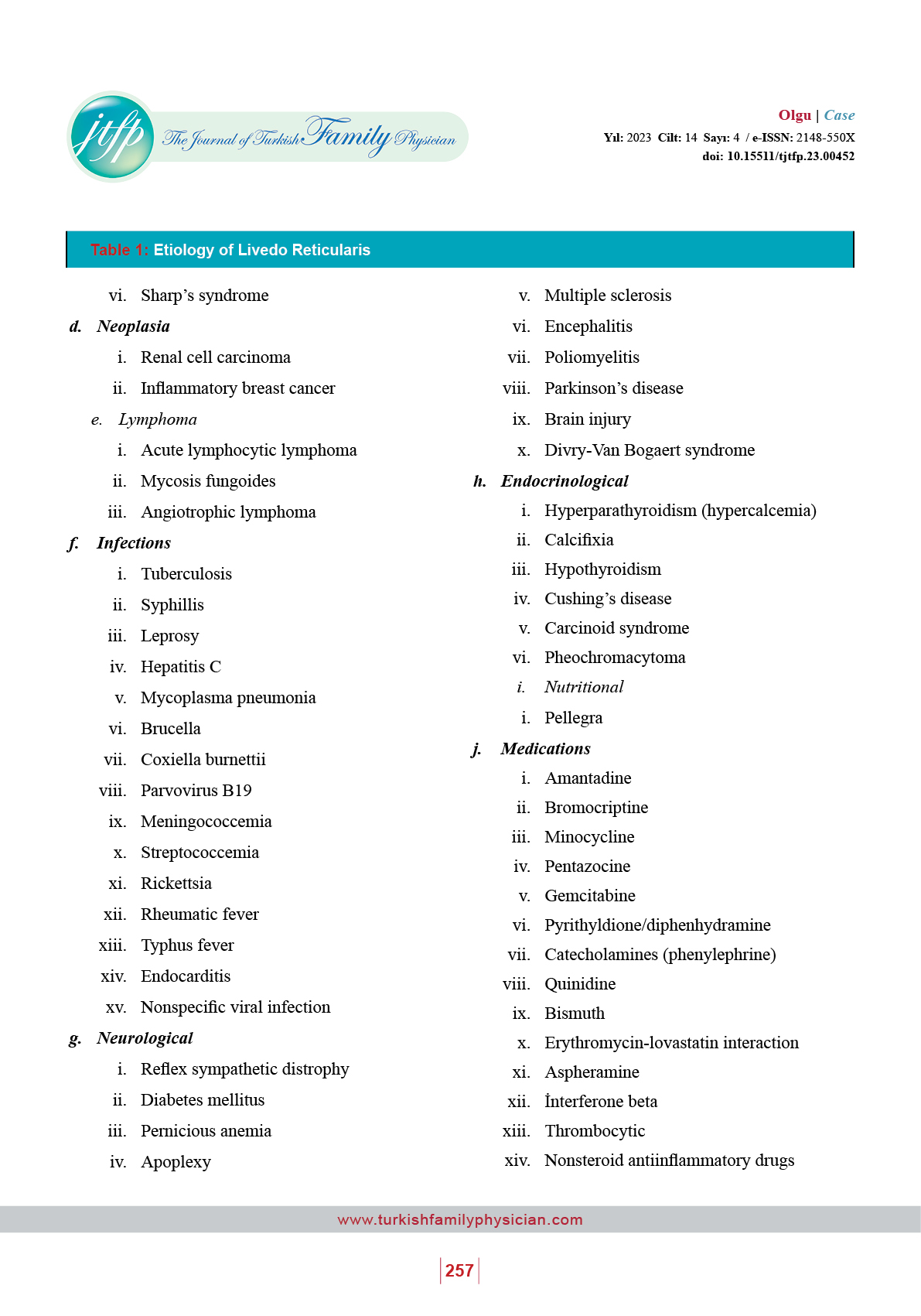
Livedo reticularis (LR), is a skin finding consisting of transient or persistent, macular, violaceous, connecting rings that form a netlike cyanotic pattern.(1-2) This appearence may be caused by any situation which is related to increase of visibility of the venous plexus under the dermal layer. Thinning of the dermis in elderly people is one of the causes of this lesion without any pathology. Venodilation (triggered by hypoxia or autonomic dysfunction) and blood deoxygenation (ie. venous thrombosis, vasospasm or increased blood viscosity) are two major causes of venous plexus visibility. Although, in most cases livedo reticularis is a result of a physiological response to cold exposure, it can also be a cutaneous sign of an underlying disease such as antiphospholipid syndrome or Sneddon’s syndrome (Table 1).(2-5)
In this paper, we present a primary LR case exacerbated by physical activity. Due to its transient nature, and the absence of additional symptoms such as pain or itching, this is a condition that is particularly challenging to diagnose. Therefore, recognition of livedo reticularis and the detection of any underlying pathology through differential diagnosis become crucial in primary care settings serving patients of all age groups.
Case
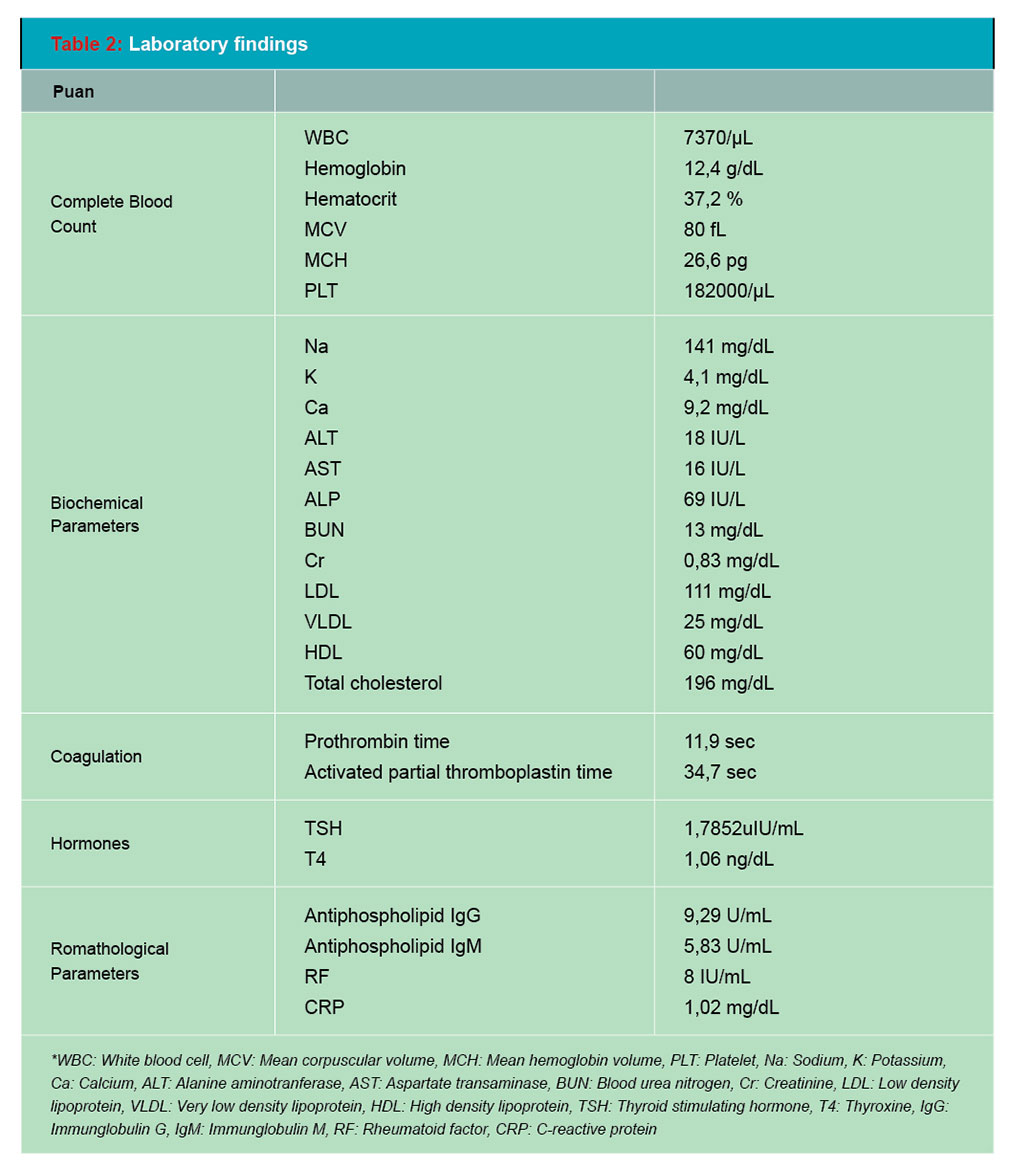
A female, 40 year old patient referred to cardiology clinic with symptoms of palpitation, mild dyspnea and fatigue. After normal physical examination findings; a complete blood count, biochemical parameters, treadmill stress test and echocardiography were planned (Table 2).
During treadmill stress test; remarkable purple, netlike, macular lesions regionally appeared on her arms and lower legs (Figure 1). She mentioned that these lesions were appearing after any physical activity and were disappearing in approximately 15 minutes. The lesions did not blanch on applying pressure and extremities were neither cold nor painful. We investigated the details of the medical history and broadened laboratory parameters to search a clue of an underlying disease. She mentioned that these lesions may appear especially when walking fast or engaging in intense household activities and disappear after a rest of 15-20 minutes in her daily life. She didn’t notice any correlation between the lesions and hot or cold temperatures.
There was no history of any precipitating factors, drug intake, chronic disease or peripheral vascular disease. She had one spontaneous abortion and two children with no obstetric complications. She had past history of tuberculosis 20 years ago. There was no similar condition or any known circulatory disorder in her family history.
Laboratory findings revealed decreased platelet co-unt, elevated lactate dehydrogenase, erythrocyte sedimentation rate and fasting plasma glucose. Activated partial thromboplastin time and prothrombin were normal. Serum electrolytes, thyroid function parameters and renal function tests were within the normal range. Echocardiogram was reported as mild aortic and tricuspid regurgitation. Anticardiolipin antibody IgG, IgM and lupus anticoagulant tests were negative. After consulting with the dermatologist we excluded possible systemic causes of livedo reticularis and we concluded to primary LR.
Discussion
Livedo reticularis is a skin finding which may be classified in two major groups: related with a systemic condition or without any systemic association. If no underlying disease is found (such as hypercoagulability, hypothyroidism, connective tissue diseases, autoimmunity or neoplasia); the situation may be physiological, primary or idiopathic.(2)
Physiological LR (or cutis marmorata) is mainly a condition of young women and is a result of the impaired blood flow in cutaneous vessels due to cold exposure. Primary LR is also a transient skin colour change but it differs from physiological one with its lack of any connection to temperature. Idiopathic LR is persistent and unresolving form and the diagnosis is reached when no other pathological signs except LR are found.(1-2)
To diagnose this situation, the most important part of the workup is to exclude any underlying pathology. The laboratory studies directed by history and physical examination are sufficient in evaluation for most of the cases. This process involves a detailed anamnesis with information regarding the use of medication, time of onset, associated symptoms, current diseases and recent surgeries. The physical examination is extremely important, as well as laboratory tests and histopathological examination that may suggest the etiology.(6)
Alhough LR is a relatively common condition, what proved interesting about our case is that it was ralated to strenuous exercise. Exercise is recommended for the treatment of LR because increased circulation helps to dilate the blood vessels throughout the body.(7) However, it is contraversial as in this case exercise was what exacerbated the situation. In this context; in the absence of an underlying cause or trigger it would be useful to consider that the condition may be associated with exercise in individuals presenting with similar complaints to a primary care physician.
Informed consent: Written informed consent was obtained from the patient for the case report and publication of the accompanying analyzes (26.05.2023).
Conflict of interest: The authors declared no conflict of interest. The authors declared that they received no financial support for this study.
Author Contributions: All authors; declared that they participated in the design, supervision, analysis and/or interpretation, literature search, writing and references.
References
- Gibbs MB, English JC 3rd, Zirwas MJ. Livedo reticularis: an update. J Am Acad Dermatol. 2005;52(6):1009-19.
- Sajjan VV, Lunge S, Swamy MB, Pandit AM. Livedo reticularis: A review of the literature. Indian Dermatol Online J. 2015 Sep-Oct;6(5):315-21.
- Dean SM. Livedo reticularis and related disorders. Curr Treat Options Cardiovasc Med. 2011 Apr;13(2):179-91.
- Silva SB1, Miot HA. Case for diagnosis. An Bras Dermatol. 2012 Mar-Apr;87(2):319-21.
- Kraemer M, Linden D, Berlit P. The spectrum of differential diagnosis in neurological patients with livedo reticularis and livedo racemosa. A literature review. J Neurol. 2005;252:1155-66.
- Quaresma MV, Gomes AC, Serruya A, Vendramini DL, Braga L, Buçard AM. Amantadine-induced livedo reticularis: Case report. An Bras Dermatol. 2015 Oct;90(5):745-7.
- Muekusch G, Pitman J. Livedo reticularis. Dermatol Nurs. 2004 Apr;16(2):181.


