Gebelerin kişilik özelliği ve stresle başa çıkma tutumlarının doğum korkusuna etkisi
Giriş ve amaç: Gebe kadınların kişilik özellikleri ve stres ile başa çıkma tutumları doğum korkusu yaşamalarını etkileyebilmektedir. Bu araştırma gebelerin kişilik özelliği ve stresle başa çıkma tutumlarının doğum korkusuna etkisini değerlendirmek amacıyla yapılmıştır.
Yöntem: Tanımlayıcı tipte olan bu araştırma Ekim 2017-Mart 2018 tarihleri arasında bir kamu hastanesinin gebe polikliniklerine başvuran 416 gebe ile yapılmıştır. Veriler; Gebe Tanıtım Formu, On-Maddeli Kişilik Ölçeği (OMKÖ), Stresle Başa Çıkma Tutumları Envanteri (SBTE) ve Wijma Doğum Beklentisi / Deneyimi Ölçeği A Versiyonu (W-DEQ V-A) ile elde edilmiştir. İstatistiksel değerlendirmede; sayı, yüzde, ortalama, standart sapma ve Pearson korelasyon analizi kullanılmıştır.
Bulgular: Yaş ortalaması 28,80±5,89 olan gebelerin %34,1’inin ilköğretim mezunu olduğu, %79,1’inin çalışmadığı ve %78,1’inin gelirinin giderine denk olduğu saptanmıştır. W-DEQ V-A toplam puan ortalaması 68,39±23,60 olarak bulunmuştur. W-DEQ V-A toplam puan ortalaması ile OMKÖ dışadönüklük, duygusal dengelilik, deneyimlere açıklık, sorumluluk ve yumuşak başlılık alt boyutları arasında negatif yönde düşük düzeyde anlamlı ilişki bulunmuştur (r= -0.103, -0.219, -0.161, -0.134, -0.157; p<0.05). W-DEQ V-A toplam puanı ile SBTE dine sığınma, dış yardım arama, kaçma duygu-saleylemsel ve kaçma biyokimyasal alt boyutları arasında negatif yönde düşük düzeyde anlamlı ilişki bulunmuştur (r= -0.111, -0.223, -0.182, -0.147; p<0.05).
Sonuç: Negatif kişilik özelliklerine sahip ve stresle baş etmekte güçlük çeken gebelerin doğum korkusunu daha şiddetli yaşadıkları belirlenmiştir.
Tam Metin
Background and Aim
Childbirth is a multidimensional process with emotional, physical, physiological, social, cultural, and mental dimensions, which is considered a critical experience in every woman’s life.(1) Fear of childbirth (FoC) defined as the fear before, during and after birth. In addition to this definition FoC in literature is defined as negative cognitive birth perception and approach to birth with fear and anxiety.(2,3) According to researches carried out in many countries, approximately 20 to 80 per cent of pregnant women experience differing levels of FoC, and the incidence of FoC has increased over time.(4) Researches demonstrate that approximately 25% of pregnant women suffer from a high level of FoC.(5)
Pregnants personality traits and their psychological characteristics are effective on their thoughts, emotions and expectations in pregnancy.(6,7) With limited number of researchs on the subject, women with FoC were also more anxiety prone, more short tempered and antisocial than women with no FoC.(8) Women who have personality disorders and emotional instability and in terms of physically and emotionally childlike traits experience more difficulty in pregnancy.(6) In addition stress perception varies according to the personality characteristics in pregnants.(9) A number of changes in the pregnancy, life style, roles, relationships and responsibilities of women cause stress.(7,10) and the ability of the woman to cope with the stressful sitituations may affected by in particular her personality conditions and emotional stability.(10)
Increasingly strong evidence points to many negative consequences of stress, such as failure to maintain optimal health behaviors in pregnancy.(11) When pregnants experience stress, their body produce more cortisol. This situation adversely affects the immune system of pregnants and the health of the fetus and chronic stress over the course of a few weeks may slow fetal development and result in future problems in the child.(4,7) In the literature, women with a stressful pregnancy period also have more FoC.(5,7) and when they can not cope with stress effectively, negative consequences of stress may threaten maternal and fetal health.(7,9,12)
Consequently it can be said that when pregnant women have negative personality traits and cannot cope with stress sufficiently, they can experience severe FoC. When the related literature is examined, there are many researches explored the effect of personality traits of pregnant women on FoC(8,13-17) and few researches have been found regarding the relationship between coping methods of pregnant women and FoC.(18,19) but there are no researches investigating the effect of personality traits and stress coping methods for pregnant women on the FoC.
Therefore by determining pregnants’ negative personality traits and their poor coping abilities are important to decrease their level of FoC, and its negative consequences on maternal-fetal health. In the light of this information, this research was conducted to determine the effect of personality traits of pregnants and their ways of coping with stress on the FoC.
Materials and Methods
Design
The descriptive research was conducted between October 2017 and March 2018 in the antenatal outpatient clinics of a public hospital in eastern Turkey.
Participants and Procedure
The population of the research consisted of 28850 pregnant women who were admitted to antenatal outpatient clinics in 2017 and in the third trimester (28-40 weeks of gestation). Sample size was calculated as 416 pregnant with 5% level of significance, 95% confidence interval and 80% ability to represent the population. The pregnant women who accepted to participate in the research were selected from the patient record system with random sampling method. The data were obtained by the researchers on the weekdays in the mentioned hospital by using face-to-face interview method.
Criteria of inclusion for pregnant women- Being in the third trimester of pregnancy- Planning to have normal birth- Not having communication problems- Volunteering to take part in the study Criteria of exclusion for pregnant women- Having history of cesarean section- Having pregnancy related complications
Data Collection Tools
Pregnant Identification Form: This form consists of 15 questions in order to determine some sociodemographic (age, education level, occupation etc.) and obstetric characteristics (pregnancy week, gravida etc.) of the pregnant women. Ten-Item Personality Inventory (TIPI): This scale consists of ten items and developed by Gosling et all measures five important personality traits, including openness to experience, agreeableness, extraversion, conscientiousness and emotional stability. It was adapted to Turkish culture by Atak (2013) and has seven point likert scale and there are two items in each sub-dimension. The internal consistency values of the sub-dimensions of scale ranged from 0.81 to 0.86.20 In this research, internal consistency values of the sub-dimensions varies between 0.75 and 0.79.
Inventory for Coping With Stress Attitudes (ICSA): The purpose of the inventory developed by Özbay (1993)(21) and adapted to Turkish by Özbay and Şahin (1997)(22) is to determine the coping attitudes of individuals in different stress situations. 5 point Likert type scale has 43 items and six sub-dimensions. These are inclining towards religion, looking for outside help, active planning, escape-isolation (emotional-operational), escape-isolation (bio-chemical) and acceptance-cognitive. The internal consistency values for the sub-dimensions ranged from 0.56 to 0.89.(23) In this research, internal consistency values of the sub-dimensions varies between 0.53 and 0.68.
Wijma Delivery Expectancy/Experience Questionnaire (W-DEQ): W-DEQ developed by Wijma et al. (1998)(24) is a likert type scale consisting of 33 item which evaluating stress and FoC. Each expression is given a score of 0 to 5. The answers of those questions that are positively formulated (item numbers 2, 3, 6, 7, 8, 11, 12, 15, 19, 20, 24, 25, 27, 31) have to be reversed for the calculation. The cut off point of the scale is 84 and a higher score indicates a more intense FoC. W-DEQ fear of childbirth levels are classified as; those who have a low FoC (W-DEQ score ≤ 37), those who have a moderate FoC (those with a W-DEQ score of 38-65), those who have a severe FoC (W-DEQ score 66-84) and those who have a clinical FoC (W-DEQ score ≥ 85). The scale was adapted to Turkish by Körükçü and Kukulu (2012) and internal consistency value of the scale is 0.89.(25)In this research, internal consistency value of the scale was found as 0.91.
Data Analysis
Data were analyzed by in the computer environment using SPSS 16.0 package software (SPSS Inc, Chicago, IL). Percentage distribution, arithmetic mean, standard deviation and Pearson correlation tests were used in statistical evaluation. Statistical significance level was accepted as p<0.05. Ethical ConsiderationIn order to conduct the research, approval was received from the Health Sciences Non-Interventional Clinical Research Ethics Committee of Inönü University (Decision No: 2017/22-9). Additionally, written permission was received from the institutions. Before starting the research, the participants were informed about it and those who volunteered were included in the research.
Results
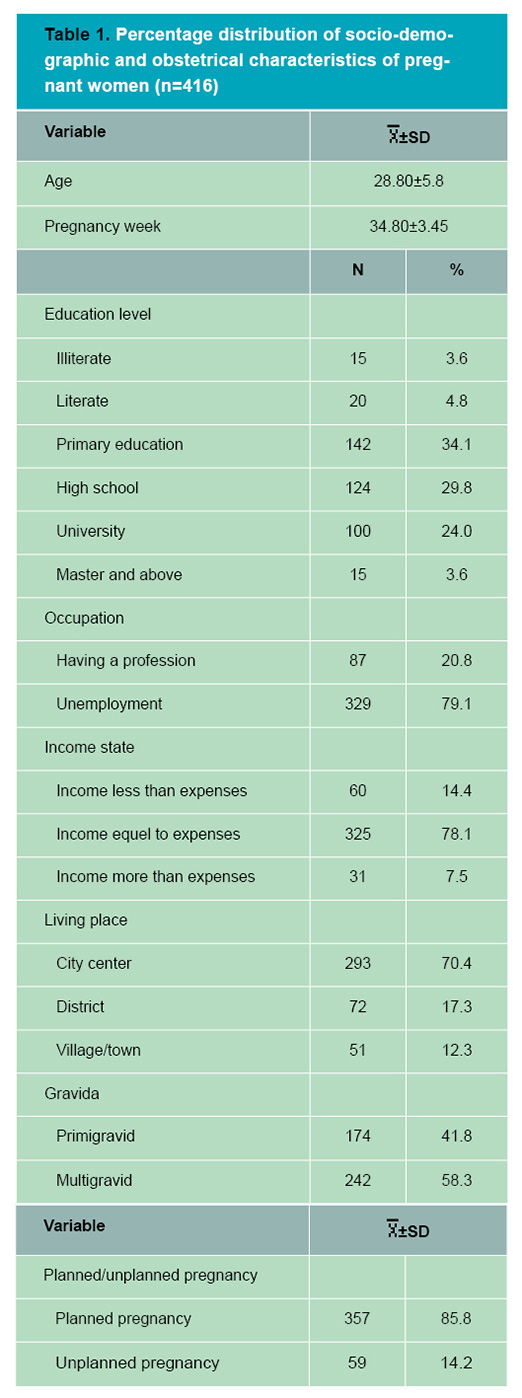
34,1% of pregnants with a mean age of 28,80±5,89 were primary graduates, 79,1% were unemployment, 78,1% were equal to the expenses of their income and 70,4% were living in the city center. Also; 58,3% of the pregnant women were multigravid and 85,8% of them had planned pregnancy (Table 1).
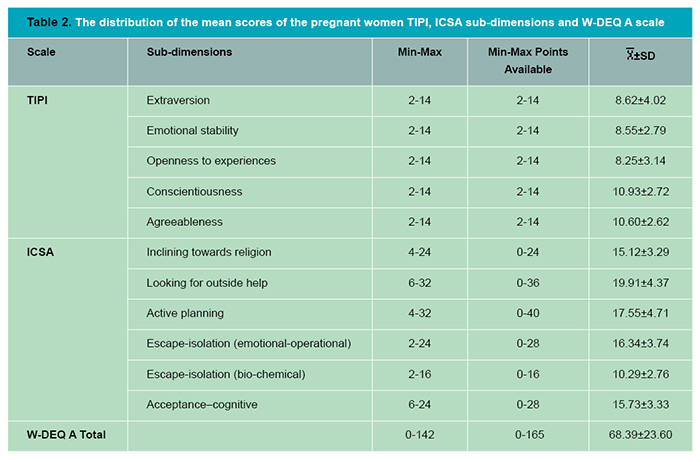
The mean score of TIPI extraversion sub-dimension of pregnant women was 8.62± 4.02, emotional stability sub-dimension was 8.55±2.79, openness to experiences sub-dimension was 8.25±3.14, conscientiousness sub-dimension was 10.93±2.72 and agreeablenes sub-dimen-sion was 10.60±2.62 respectively. The mean score of ICSA inclining towards religion was 15.12±3.29, looking for outside help sub-dimension was 19.91±4.37, active planning sub-dimension was 17.55±4.71, escape-isolation (emotional-operational) sub-dimension was 16.34±3.74, escape-isolation (bio-chemical) sub-dimension was 10.29±2.76 and acceptance–cognitive sub-dimension was 15.73±3.33 respectively. In addition, the mean total score of the W-DEQ V-A scale was 68.39± 23.60 (Table 2).
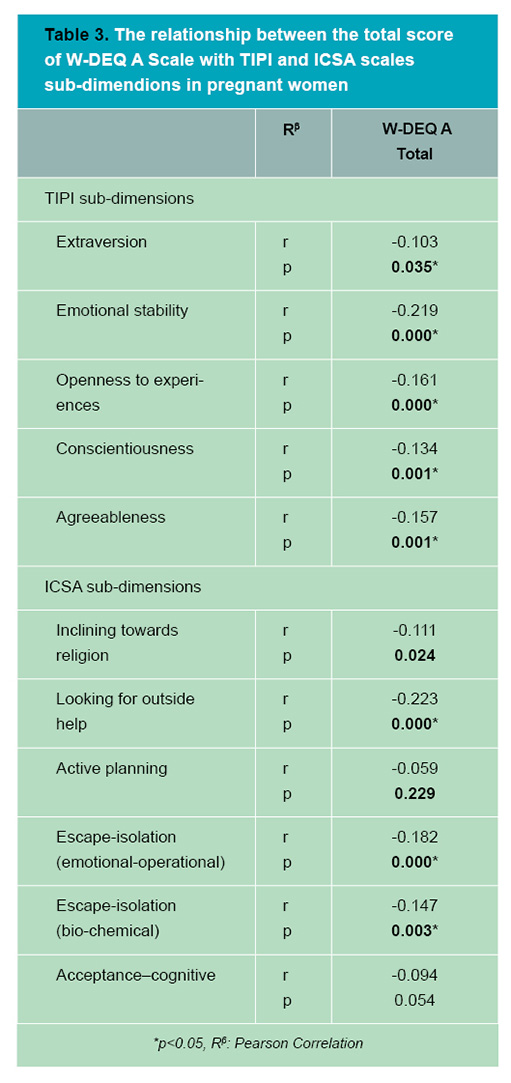
A significant low-level correlation was found between the W-DEQ V-A mean total score of the pregnant women and TIPI extraversion, emotional stability, opennes to experiences, conscientiousness and agreeableness sub-dimensions (respectively r = -0.103, p<0.035; r = -0.219, p<0.000; r = -0.161, p<0.000; r = -0.134, p<0.001; r = -0.157, p<0.001).
There was a low negative correlation between W-DEQ V-A total score and ICSA inclining towards religion, looking for outside help, escape-isolation (emotional-operational) and escape-isolation (bio-chemical) (respectively r = -0.111, p<0.024; r = -0.223, p<0.000; r = -0.182, p<0.000; r = -0.147, p<0.003) (Table 3).
Discussion
In our research pregnant women W-DEQ V-A scale average score was 68.39±23.60. Similarly, Körükçü et al (2017) in their research the average score of W-DEQ V-A was 79.95±17.33.(26) Sahin et al (2009) found that the average score of W-DEQ V-A was 85.63±13.76 and the FoC was high in pregnant women.(27)
A significant low-level correlation was found between the W-DEQ V-A mean total score of the pregnant women and TIPI extraversion, emotional stability, opennes to experiences, conscientiousness and agreeableness sub-dimensions (p<0.05). It has been observed that the FoC increases significantly with increasing tendency to negatif personality traits in all sub-dimensions. FoC is higher in women who have high levels of anxiety, anxious, often have negative thoughts, always think they are unlucky, dissocial, pessimistic and have negative superstitious beliefs about pregnancy.(8,13,18,28)
Johnson et al (2013) found that in their research of maternal trait personality and childbirth the characteristics of extraversion and emotional stability in women increased the likelihood of normal birth.(29) Handelzalts et al (2012) found that the FoC is associated with emotional instability, anxiety sensitivity and low level of responsibility of pregnants.(8) In addition Conrad and Strickerb (2017) stated that mothers who scored low on extraversion and emotional stability were more likely to have a negative experience, including increased rates of caesarean sections and birth complications.(30)
Ryding at al (2007) in their research which evaluated the relationship between personality and FoC the women who had sought help tended to be more anxiety-prone, more short-tempered, and lower in socialisation. In spite of counselling, they reported more intense fear of delivery and fear of pain compared with the comparison group.(14) It is seen that the findings are consistent with the literature and personality trait is a factor related to FoC. When evaluated in this respect, it may be said that pregnants who extraversion, emotional balanced, open to new experiences, conscientiousness and agreeableness experience less FoC.
When the relationship between the FoC and the coping ways of the pregnant women with stress were evaluated as the level of FoC increased there was a significant decrease in the ways of coping inclining towards religion, looking for outside help, escape-isolation (emotional-operational) and escape-isolation (bio-chemical) sub-dimensions (p<0.05). This finding may interpret as pregnants who inclining to religion, looking for outside help for coping with stress and have avoidance behavior experience less FoC. Women who experience risk in pregnancies can benefit from inclining to religion (spirituality) for their themselves and their unborn children.(31)
Bhat et al (2015) stated that religious coping methods seems to contribute to a better understanding of the stressful process that pregnant women experience and the positive forms of religious coping methods that includes emotions like feeling well in pregnant women generally gives positive outcomes and the negative forms of religious coping methods feeling like sinful and abandoned, often leads to negative outcomes.32 In Guardino ve Dunkel Schette (2014) systematic review pregnants avoidant coping behaviors or styles and poor coping skills in general are associated with their low psychological well-being, distress, high depressive mood, high anxiety and high stress level during pregnancy.(11)
In the literature, the researches eveluating the relationship between FoC and coping with stress is limited. In the qualitative research of Nieminen et al. (2015) they evaluated the nulliparous attitudes to imminent childbirth before and after an 8-week program internet-based cognitive behavioral therapy for severe FoC. They observed that before therapy the basic method of coping with the FoC was avoidance in nulliparous and after the therapy they mostly used active participation method substitute of avoidance.(33)
In the literature, it is also emphasized that strong personality traits and previous experiences related to stressful situations reduce the effect of stress that may occur due to pregnancy.(18) In this respect, it can be said that lack of coping methods with stress effectively may lead to severe FoC in pregnant women.
In conclusion, the results of the research could be useful for midwifery practice. According to finding from this research FoC is associted with negative personal traits of pregnants and their ability to cope with stressful situations. For this reason, it is important to take into consider women personal traits and enhance their coping abilities to reduce the FoC effectively in antenatal care.
Limitations: This research is limited to the pregnant women who visited antenatal outpatient polyclinics of a state hospital located in the east of Turkey.
Acknowledgements: We would like to thank the pregnant women who participated in and completed this questionnaire.
Conflict of Interest: The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Referanslar
- Soltani, F, Eskandari Z, Khodakarami B, Parsa P, Roshanaei G. Factors contributing to fear of childbirth among pregnant women in Hamadan (Iran) in 2016. Electronic Physician 2017;9(7):4725-31.
- Çiçek Ö, Mete S. A common problem: fear of childbirth. DEUHFED 2015;8(4):263-8.
- El-Aziz SNA, Mansour SES, Hassan NF. Factors associated with fear of childbirth: It’s effect on women’s preference for elective cesarean section. J Nurs Educ Pract 2017;7(1):133-45.
- Lopukhovaa OG, Kashshapovab EV. Fear of childbirth in pregnant women: external and internal factors. Psychology in Russia: State of the Art 2015;8(4):114-25.
- Veringa IK, Bruin EI, Bardacke N, Duncan LG, Steensel FJA, Dirksen CD, Bögels SM. ‘I’ve changed my mind’, mindfulness-based childbirth and parenting (MBCP) for pregnant women with a high level of fear of childbirth and their partners: study protocol of the quasi-experimental controlled trial. BMC Psychiatry 2016;16(377):1-14.
- Babacan GA, Çevik N, Hataf HS, Biçen Ş, Keskin G, Tuna MA. Characteristics associated with self-esteem and body image in pregnancy. Anatol J Clin Investig 2011;5(1):7-14.
- Atasever İ, Sis ÇA. Effect of prenatal stress on maternal- child health. Journal of Anatolia Nursing and Health Sciences 2018;21(1):60-8.
- Handelzalts JE, Fisher S, Lurie S, Shalev A, Golan A, Sadan O. Personality, fear of childbirth and cesarean delivery on demand. Acta Obstet Gynecol Scand 2012;91(1):16-21.
- Elkin N. Ways of coping with stress affecting factors of pregnant women. Mersin Univ Journal of Health Sciences 2015;8(1):22-31.
- Tyrlika M, Konecny S, Kuklac L. Predictors of pregnancy-related emotions. J Clin Med Res 2013;5(2):112-20.
- Guardino CM, Schetter CD. Coping during pregnancy: a systematic review and recommendations. Health Psychol Rev 2014;8(1):70–94.
- Klabbers GA, van Bakel HJA, van den Heuvel MMA, Vingerhoets AJJM. Severe fear of childbirth: its features, assesment, prevalence, determinants, consequences and possible treatments. Psychological Topics 2016;25(1):107-27.
- Saistoa T, Salmela-Arob K, Nurmic JE, Èkia EH. Psychosocial characteristics of women and their partners fearing vaginal childbirth. BJOG 2001;108:492-8.
- Ryding EL, Wirfelt E, Wangborg IB, SjÖgren B, Edman G. Personality and fear of childbirth. Acta Obstetricia et Gynecologica 2007;86:814-20.
- Tekinarslan E. Gebelerde d-tipi kişilik özelliğinin normal doğum korkusu üzerine etkisi. Dissertation, 2015. Selçuk University Medical Faculty, Department of Psychiatry, Konya.
- Dursun E. Gebelerin kişilik özellikleri ve kaygı düzeyleri ile doğum korkuları arasındaki ilişki. Master’s Thesis, 2018. Hacı Bektaş Veli University, Institute of Science Department of Nursing, Nevşehir.
- Gönenç İM, Aker MN, Güven H, Moraloğlu TÖ. The effect of the personality traits of pregnant women on the fear of childbirth. Perspectives in Psychiatric Care 2019. https://doi.org/10.1111/ppc.12440, aderesinden 23/06/2019 tarihinde erişilmiştir.
- Melender HL. Fears and coping strategies associated with pregnancy and childbirth in J Midwifery Womens Health 2002;47(4):256-63.
- Greer J, Lazenbatt A, Dunne L. ‘Fear of childbirth’ and ways of coping for pregnant women and their partners during the birthing process: a salutogenic analysis. The Royal College of Midwives. Evidence Based Midwifery 2015;12(3):95-100.
- Atak H. The Turkish adaptation of the ten-item personality inventory. Archives of Neu ropsychiatry 2013;50:312-9.
- Özbay Y. An investigation of the relationship between adaptational coping process and self-perceived negative feelings on international students. PhD Thesis, 1993. Texas Tech University, Lubbock, Texas.
- Özbay Y, Şahin B. Stresle başa çıkma tutumları envanteri: Geçerlik ve güvenirlik çalışması. 4. Ulusal Psikolojik Danışma ve Rehberlik Kongresi Bildirisi, 1997. Ankara.
- Önen AS. The effects of student teachers’ personality traits & EQ levels on stress coping. Hacettepe University Journal of Education 2012;42:310-20.
- Wijma K, Wijma B, Zar M. Psychometric aspects of the W-DEQ; a new questionnaire for the measurement of fear of childbirth. J Psy-chosom Obstet Gynecol 1998;19:84-97.
- Körükcü Ö, Kukulu K, Fırat MZ. The reliability and validity of the Turkish version of the wijma delivery expectancy/experience questionnaire (W-DEQ) with pregnant women. Journal of Psychiatric and Mental Health Nursing 2012;19(3):193-202.
- Körükçü Ö, Deliktaş A, Aydın R, Kabukcuoğlu K. Investigation of the relationship between the psychosocial health status and fear of childbirth in healthy pregnancies. Clin Exp Health Sci 2017; 7:152:8.
- Şahin N, Dinç H, Dişsiz M. Pregnant women’s fear of childbirth and related factors. Medical Bulletin of Zeynep Kamil 2009;40(2):57-62.
- Nilsson C, Lundgren I, Annika KA, Hildingsson I. Self reported fear of childbirth and its association with women’s birth experience and mode of delivery: A longitudinal population-based stud. Women and Birth 2012;25:114-21.
- Johnson RG, Brown AE. Maternal trait personality and childbirth: The role of extraversion and neuroticism. Midwifery 2013; 29(11):1244-50.
- Conrad M, Stricker S. Personality and labor: a retrospective study of the relationship between personality traits and birthing experiences. J Reprod Infant Psychol 2017:1-14.
- Price S, Lake M, Breen G, Carson G, Quinn C, OConnor T. The spiritual experience of high-risk pregnancy. JOGNN 2007;36(1):63-70.
- Bhat NA, Hassan R, Shafiq M. Religious coping and adjustment among pregnant women. Annals of Biological Research 2015,6(6):39-47.
- Nieminen K, Malmquist A, Wijma B, Ryding E-L, Andersson G, Wijma K. Nulliparous pregnant women’s narratives of imminent childbirth before and after internet-based cognitive behavioural therapy for severe fear of childbirth: a qualitative study. BJOG 2015;122:1259–65.


