Hastalık hakkında bilgilendirmenin COVID-19 vakalarında kaygı düzeyi üzerine etkisi
Giriş: Bu çalışmanın amacı, karantina sürecinde Covid-19 hastalarını hastalık hakkında bilgilendirmenin ve takip etmenin kaygı düzeylerine etkisini belirlemektir.
Gereç ve yöntem: Bu çalışmaya, 1 Ağustos – 30 Eylül 2020 tarihleri arasında İstanbul Tuzla’da ev izolasyonunda izlenen 18-65 yaş arası Covid-19 hastaları dahil edildi. Test sonuçlarını bildirmek için yapılan telefon görüşmesinde sosyodemografik bilgileri kaydedildi. Durumluk Kaygı Ölçeği (STAI-I), Hasta Sağlığı Anketi-4 (PHQ-4) ve Koronavirüs Anksiyete Ölçeği (CAS) uygulandı. Ev ziyaretleri düzenlenerek hastalara enfeksiyonun seyri, izolasyon ve tedavisi hakkında bilgi verildi. Hastalar gün aşırı telefon görüşmeleri ile takip edildi. Hastalara izolasyonun 11. gününde aynı anketler uygulandı, skorlar ilk sonuçlarla karşılaştırıldı.
Bulgular: Çalışmaya dahil olan 98 katılımcının 50’si kadın (%51), 48’i erkekti (%49). İlk görüşmedeki ve 10. gün sonundaki ortalama puan dikkate alındığında; STAI-I skorları anlamlı olarak azaldı (p<0,001). Bu azalma kadınlarda ve ilkokul mezunlarında daha yüksekti (sırasıyla p<0,001 ve p=0,010). PHQ-4 ve CAS skorları arasındaki değişim istatistiksel olarak anlamlı değildi (sırasıyla p=0,319 ve p=0,053).
Sonuç: Yeterli bilgilendirme ve düzenli takip hastaların yalnızlık ve çaresizliklerini azaltarak anksiyete ile baş etmede etkilidir.
Tam Metin
Introduction:
In the outbreak of SARS-Cov-19 (Covid-19), which was called a pandemic by the World Health Organization in January 2020, countries started to take various measures, especially social isolation.(1) In addition, the news about Covid-19 cases and the high mortality rates announced, both in the social media and in the press, caused a great concern in the society.(2,3) While uncertainties in treatment and prognosis increase anxiety in the general population; difficulties in hospital services have been the main factors triggering anxiety in those with chronic diseases, isolation and limitations in certain age groups, and intense and risky work tempo, especially in healthcare workers.(4-8)
Within the scope of epidemic control measures in Turkey, filiation studies started from the first days, cases and their close contacts were quarantined and home isolation was ensured.(9) In the current practice, if the patients who have had PCR test do not have an indication for hospitalization, these people learn the test results from the electronic health tracking system (E-Nabız) or by calling from the district health directorates at home.
In the first contact, the short medical history of the person and the people with whom he was in contact are learned and recorded, and then the medicine that is approved by the district health directorate doctor is delivered to them by teams. During the next isolation period, the patient’s follow-up is left to the family physician. The aim of our study is to reveal the effect of effective information about the course, treatment and isolation process of Covid-19 and then regular medical follow-up on the level of anxiety in patients.
Materials And Methods:
The study was conducted with the Covid-19 positive cases between the ages of 18-65 who were found in Tuzla, Istanbul between 1 August and 30 September 2020 and were suitable for home follow-up. Exclusion criteria of the study were currently being treated for any acute or chronic illness other than Covid, having a history of anxiety or depression, and being hospitalized for Covid-19 treatment. Of the patients registered in the follow-up programme, 128 people met the study criteria.
The sample size was calculated as 96 people at 95% confidence level, and it was aimed to reach 100 patients for the study. The data of 98 patients were recorded due to the worsening of the medical condition of 2 patients who were referred to the hospital. The identified patients were followed up by periodic phone calls of a single contact tracing team.
In this way, it was aimed to provide standardization in practice. After the test results were reported in the first interview of the patients; their sociodemographic information was recorded, and the State Anxiety Inventory (STAI-I), the Patient Health Questionnaire-4 (PHQ-4) and the Coronavirus Anxiety Scale (CAS) were applied to them. Then, the team, who made the phone call, organized a home visit, delivered the medicines to the patient and informed the people about the characteristics of the Covid-19 infection, the course of the disease, the isolation and treatment. In the meantime, the Ministry of Health Covid-19 brochures were delivered.
The patients were evaluated by phone calls every other day and their follow-up was carried out. The questions of the patients in isolation were answered and they were provided to communicate with the social support units if they needed it.
During the period of the study, the isolation duration of the patients was determined as 14 days by the Ministry of Health, and retesting was not applied at the end of the isolation. For this reason, the 11th day for the second survey application was chosen because it was the penultimate interview day in the follow-up of the patients. During the conversation on the 11th day of isolation, the patients were re-administered with STAI-I, PHQ-4 and CAS by the same team; and the results were recorded.
STAI-I: It is the subsection of the State and Trait Anxiety Inventory, which was developed by Spielberger et al. and whose Turkish validity and reliability was analyzed by Öner and Le Compte. It consists of 20 questions (10). State anxiety items include: “I am tense”, “I am worried”, “I feel calm”, “I feel secure”. The answers for items 3, 4, 6, 7, 9, 12, 13, 14, 17, 18 are scored positively (increasing the total anxiety score); for items 1, 2, 5, 8, 10, 11, 15, 16, 19, 20 are scored negatively (reducing the total anxiety score). Thus, the total score varies between 20-80. A high score is associated with high anxiety.
PHQ-4: The Turkish validity and reliability of this scale, which was developed by Kroenke et al., was examined by Demirci and Ekşi.(11,12) It consists of four questions and assesses psychological stress. Each question is scored between 0-3. According to the total score, 0-2 points reflect none, 3-5 points mild, 6-8 points moderate, 9-12 points serious psychological stress.
CAS: The original of the scale was developed by Lee, and Turkish reliability and validity studies were conducted (13,14).. Questions in the scale are scored between 0-4. It is reported that anxiety is high in those with a total score of 9 and above. IBM SPSS Statistics 22.0 (IBM SPSS, Turkey) program was used for statistical analysis. In the analysis of the data, the mean ± standard deviation (SD) was given if the continuous variables were normally distributed, and the median value was given if they were not normally distributed. Categorical variables were expressed as percentages.
The Repeated Measures ANOVA method was used to compare the means of continuous variables at two different times. Repeated Measures were covariantly included in the ANOVA analysis to detect categorical variables that affect the mean changes in two different times. Statistical significance was tested at the alpha=0.05 level. Ethics committee approval of the study was received on 24.07.2020 (protocol code: 09.2020.867). There is no conflict of interest in our study. No financial support was received for this study.
Results:
Of the 98 patients included in the study, 50 (51%) were female and 48 (49%) were male. The mean age is 49, with a range of ages between 21 and 62. Of the patients, 38 (38.77%) were primary school graduates, 34 (34.69%) were high school graduates, and 26 (26.53%) were graduated from a university or higher education institution. When the total scores on the first day and the 11th day were compared in the scales, it was observed that there was a decrease in all three scales. However, this decrease was found to be statistically significant only for STAI-I (Graph 1).
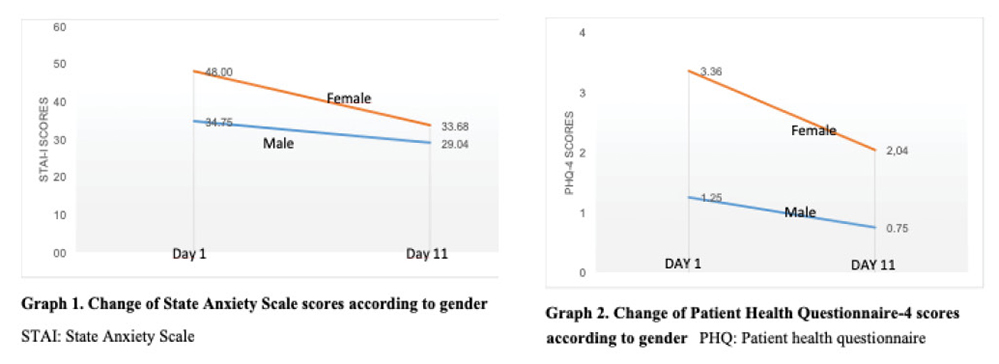
STAI-I Results: The total STAI-I score of the patients on the 11th day was statistically significantly lower than the first day (p<0.001). When gender information was included in the study as covariance, it was observed that the acceleration in women was greater than in men (p<0.001). Likewise, the rate of decrease in primary school graduates is higher (p=0.010) (Graph 1). There was no statistically significant difference when looking at acceleration according to age (p=0.452).
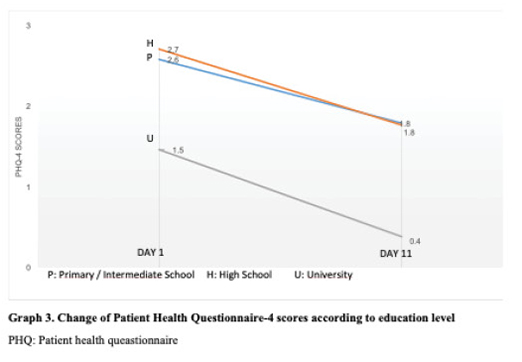
PHQ-4 Results: The difference between the mean of the scale at the time of information and the mean of the scale made after the 11th day was not found to be statistically significant (p=0.319). However, when the acceleration in the decline is examined, it was observed that the decline was faster in women and primary school graduates (p=0.010 and p<0.001, respectively) (Graph 2 and 3). No significant difference was found in terms of age.
CAS Results: The difference between the first and last day scores in terms of CAS was not statistically significant (p=0.053). In addition, the rate of decrease in the score does not show a significant difference according to gender, age and educational status (p=0.275, p=0.471 and p=0.440, respectively).
Discussion:
Health anxiety is defined as the anxiety and stress experienced by a person in the face of a situation that he perceives as a threat to health (15,16). Recently, the Covid-19 pandemic is seen as one of the main reasons that trigger health anxiety all over the world.(17) In the literature, there are studies examining the negative effects of Covid-19 on mental health and especially emphasizing the high level of anxiety.(1,18,19) Although there are studies measuring anxiety in certain age, occupation and chronic disease groups, studies measuring anxiety in Covid-19 patients are limited.(20-24) In a prospective study conducted by Parker et al., the anxiety levels of the patients at the time of admission to the hospital and after 2 weeks were compared, and similar to our study, it was observed that the anxiety decreased in the second questioning.(25)
Although in this study The Hospital Anxiety and Depression Scale (HADS) was used, the results of the research in terms of anxiety support our study results. STAI-I, PHQ-4, and CAS are scales that can be used in studies measuring anxiety due to Covid-19.(2) For example, PHQ-4 was applied in a cross-sectional study examining the effects of Covid-19 on anxiety and depression in Scotland, and as a result of this study, loneliness and lack of social support were found to increase anxiety.(26) For this reason, it is recommended to draw attention to these points in order to prevent the psychosocial consequences of the pandemic. In another study conducted with 6600 homeless people living in Hamburg, it was determined that the fear of having Covid-19 increased depression and anxiety by using the PHQ-4.(27)
In some studies measuring the relationship between Covid-19 and anxiety, STAI-I was preferred. For example, in a study conducted with women, according to the results of STAI-I, it was seen that Covid-19 anxiety was at a level that would affect the menstrual cycle.(28) In most of the studies on Covid-19 anxiety, it has been reported that female gender, young age and presence of comorbid disease increase anxiety.(29)
In our study, however, no statistically significant relationship was found between age and STAI-1 scores, while the rate of decrease in anxiety was found to be significantly higher in female gender between the first contact and the second. However, in the literature review, no prospective study was found in which 3 scales were used together and included intervention in terms of follow-up. In this respect, our study contributes to the literature.
In the interviews conducted for the study, it was seen that the reason for the anxiety in the patients was not mostly due to health concerns, based on the statements of the patients, although there were no questions on the subject in the scales. Often, patients are worried about financial problems or disruptions in the care of their relatives due to isolation. This situation reveals the effects of loneliness and isolation on anxiety, as emphasized in previous studies.(1,2) For this reason, we think that the effect of informing and monitoring on decreasing the scale scores becomes evident at this point.
A limitation of the study is that it was conducted with a small number of participants. Qualitative studies are needed to investigate the causes of anxiety associated with Covid-19. In this way, the effect of follow-up and information on reducing anxiety will be revealed with clearer data.
Conclusion:
In conclusion, Covid-19 infection is a state of high anxiety in patients. It can be said that regular follow-up and information reduce the level of general health concern and Covid-19 specific anxiety in patients.
Referanslar
- Bland AR, Roiser JP, Mehta MA, Sahakian BJ, Robbins TW, Elliott R. The impact of COVID-19 social isolation on aspects of emotional and social cognition. Cognition and Emotion 2021; 36(1):49-58. doi:10.1080/02699931.2021.1892593
- Uzunova G, Pallanti S, Hollander E. Presentation and management of anxiety in individuals with acute symptomatic or asymptomatic COVID-19 infection, and in the post-COVID-19 recovery phase. Int J Psychiatry Clin Pract 2021 Jun;25(2):115-31. doi:10.1080/13651501.2021.1887264
- Unlu U, Yıldız Çeltek N, Erdoğdu Ceylan E, Demir O. COVID-19 pandemic and vaccination from the perspective of university students: Knowledge, attitudes and practices. Euras J Fam Med 2022;11(1):75-86. doi:10.33880/ejfm.2022110110
- Cao W, Fang Z, Hou G, Han M, Xou X, Dong J et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Research 2020;287:112934. doi:10.1016/j.psychres.2020.112934
- Nelson NA, Bergeman CS. Daily stress processes in a pandemic: The Effects of worry, age, and affect. The Gerontology 2021;61(2):196-204. doi:10.1093/geront/gnaa187
- Plagg B, Engl A, Piccoliori G, Eisendle K. Prolonged social isolation of the elderly during COVID-19: Between benefit and damage. Archives of Gerontology and Geriatrics 2020;89:104086. doi:10.1016/j.archger.2020.104086
- hanafelt T, Ripp J, Trockel M. Understanding and addressing sources of anxiety among aealth care professionals during the COVID-19 pandemic. JAMA 2020;323(21):2133. doi:10.1001/jama.2020.5893
- Vanhaecht K, Seys D, Bruyneel L, Cox B, Kaesemans G, Cloet M et al. COVID-19 is having a destructive impact on health-care workers’ mental well-being. Int J Qual Health Care 2020 Dec 3: mzaa158. doi:10.1093/intqhc/mzaa158
- T.C. Sağlık Bakanlığı. Covid-19 (SARS-CoV-2 enfeksiyonu) temaslı takibi, salgın yönetimi, evde hasta izlemi ve filyasyon. https://covid19.saglik.gov.tr/Eklenti/39430/0/covid-19rehberitemaslitakibievdehastaizlemivefilyasyonpdf.pdf adresinden 22.11.2022 tarihinde erişilmiştir.
- Öner N, Le Compte A. Durumluk-Sürekli Kaygı Envanteri El Kitabı. İstanbul, Boğaziçi Üniversitesi Yayınları No:333; 1985.
- Demirci İ, Eksi H. Don’t Bother Your Pretty Little Head Otherwise You Can’t Enjoy Life.; ERPA International Congresses on Education 2018, 28 June -1 July 2018, Istanbul.
- Kroenke K, Spitzer RL, Williams JBW, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics 2009;50(6):613-21.doi:10.1176/appi.psy.50.6.613
- Lee SA. Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Studies 2020;44(7):393-401. doi:10.1080/07481187.2020.1748481
- Bi̇çer İ, Çakmak C, Demi̇r H. Koronavirüs Anksiyete Ölçeği Kısa Formu: Türkçe geçerlik ve güvenirlik çalışması. Anadolu Kliniği Tıp Bilimleri Dergisi 2020; 25: 216-25. https://doi.org/10.21673/anadoluklin.731092
- Abramowitz JS, Olatunji BO, Deacon BJ. Health anxiety, hypochondriasis, and the anxiety disorders. Behav Ther 2007;38(1):86-94. doi:10.1016/j.beth.2006.05.001
- Asmundson GJG, Abramowitz JS, Richter AA, Whedon M. Health anxiety: current perspectives and future directions. Curr Psychiatry Rep 2010;12(4):306-12. doi:10.1007/s11920-010-0123-9
- Tyrer P. COVID-19 health anxiety. World Psychiatry 2020;19(3):307-8. doi:10.1002/wps.20798
- Hayat K, Haq M, Wang W, Khan FU, Rehman AU, Rasool MF et al. Impact of the COVID-19 outbreak on mental health status and associated factors among general population: A cross-sectional study from Pakistan. Psychology, Health & Medicine 2022 Jan;27(1):54-68. doi:10.1080/13548506.2021.1884274
- Holmes EA, O’Connor RC, Perry VH, Wessely S, Arseneault L et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry 2020;7(6):547-60. doi:10.1016/S2215-0366(20)30168-1
- Hu Y, Chen Y, Zheng Y, You C, Tan J, Hu L et al. Factors related to mental health of inpatients with COVID-19 in Wuhan, China. Brain Behav Immun 2020;89:587-93. doi:10.1016/j.bbi.2020.07.016
- Iqbal Y, Al Abdulla MA, Albrahim S, Latoo J, Kumar R, Haddad PM. Psychiatric presentation of patients with acute SARS-CoV-2 infection: a retrospective review of 50 consecutive patients seen by a consultation-liaison psychiatry team. BJPsych Open 2020;6(5):e109. doi:10.1192/bjo.2020.85
- Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav Immun 2020;89:594-600. doi:10.1016/j.bbi.2020.07.037
- Nie XD, Wang Q, Wang MN, Zhau S, Liu L, Zhu YL et al. Anxiety and depression and its correlates in patients with coronavirus disease 2019 in Wuhan. Int J Psychiatry Clin Pract 2021 Jun;25(2):109-14. doi:10.1080/13651501.2020.1791345
- Zhang J, Yang Z, Wang X, Zhao S, Li J, Dong L, et al. The relationship between resilience, anxiety, and depression among patients with mild symptoms of COVID-19 in China: A crosssectional study. J Clin Nurs 2020 Nov;29(21-22):4020-9. doi:10.1111/jocn.15425
- Parker C, Shalev D, Hsu I, Shenoy A, Cheung S, Nash S et al. Depression, anxiety, and acute stress disorder among patients hospitalized with Coronavirus disease 2019: A prospective cohort study. Psychosomatics 2021 March-April; 62(2): 211–9. doi:10.1016/j.psym.2020.10.001
- Hubbard G, den Daas C, Johnston M, Dixon D. Sociodemographic and psychological risk factors for anxiety and depression: Findings from the Covid-19 health and adherence research in Scotland on mental health (CHARIS-MH) Cross-sectional survey. Int J Behav Med 2021;28(6):788-800. doi:10.1007/s12529-021-09967-z
- Hajek A, Heinrich F, van Rüth V, et al. Prevalence and determinants of depression and anxiety measured by the PHQ-4 among homeless individuals during the COVID-19 pandemic. Evidence from the Hamburg survey of homeless individuals. Psychiatry Res 2022;308:114350. doi:10.1016/j.psychres.2021.114350
- Demir O, Sal H, Comba C. Triangle of COVID, anxiety and menstrual cycle. J Obstet Gynaecol 2021;41(8):1257-61. doi:10.1080/01443615.2021.1907562
- Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord 2020;277:55-64. doi:10.1016/j.jad.2020.08.00m


