Covid-19 Pandemisi korkusu nedeniyle tanısı geciken çekum tümörü
Türkiye’de 11 Mart 2020’de başlayan COVID-19 pande-misi toplam 8,964,711 doğrulanmış vakaya ve 78,407 kişinin ise ölümüne neden oldu.72 yaşındaki olgumuz pandeminin başlaması ile şehirden kırsaldaki köy evine taşınmış. aşık 6 ay önce başlayan iştahsızlık ve karın ağrısı şikayetleri neden ile aldığı tedaviden fayda görmemiş ve takiplerine COVID-19 korkusu nedeniyle gitmemiş. Aile Sağlığı Merkezimizde yapılan fizik muayenesinde kaşektik görünüm, sağ alt kadranda şişlik ve ele gelen sert kitle nedeniyle abdominal USG yapıldı. Yapılan abdominal USG’de çekal alana uyan bölgede yaklaşık 65×58 mm’lik kitle gözlendi. Patolojik tanı orta derecede differansiye adenokarsinom olarak geldi. Tümörün genetik incelemesinde BRAF V600E/E2/D mutasyonu saptandı. Kemoterapi alan hasta remisyonda olup hala takip edilmektedir. Olgumuzu COVİD 19 pandemisi nedeniyle tanısı geciken tümör olgularına dikkat çekmek için literatür bilgileri eşliğinde sunmayı amaçladık.
Tam Metin
Introduction
Appeared first in the Wuhan State of China in late December 2019, COVID-19 infection resulted in a global pandemic. Within the period between the beginning of COVID-19 pandemic and the date of 9 December 2021, the number of confirmed cases is 267,184,623 in the world and 8,964,711 in Turkey. The number of deaths was reported to be 5,277,327 at the global scale and 78,407 in Turkey. The number of deaths was reported to be 2,930,732 at the global scale and 33,939 in Turkey.(1) Many individuals avoid applying to the medical institutions due to the pandemic. For these reasons, significant delays occurred in diagnoses and treatments of diseases.
Given the year 2018 data obtained from Turkish Statistical Institute (TÜİK), the total number of deaths due to malign tumors was reported to be 81,129. Colorectal cancer (7.8%) is the 4th most common cause of death.(2) The anatomic distribution of colorectal cancers is cecum (15%), right colon (20%), transvers colon (15%), left colon (5%), sigmoid colon (25%), and rectum (20%).(3) It was aimed to present the case together with literature in order to draw attention to tumor cases diagnosed late due to the COVID-19 pandemic.
Case Presentation
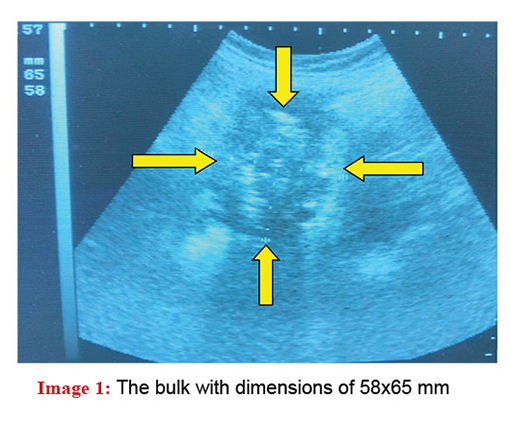
Receiving treatment for hypertension, hyperlipi-demia, and depression, our 72-year-old female patient has moved from urban to her village house 8 months ago due to the COVID-19 pandemic. The patient, whose complaints of stomachache and loss of appetite started approx. 6 months ago, received treatment for peptic ulcer activation and irritable bowel syndrome diag-nosed in the healthcare facility she has applied to. She applied to our family healthcare center due to increases in complaints of weight loss (approx. 15 kg), weariness, and loss of appetite. In the inspection, there was a hard and small swelling, which has cachectic appearance, in the right lower quadrant of abdomen. During the palpation, an unmovable hard bulk with dimensions of 6×5 cm was found. Subsequently, abdominal USG performed in our department showed that there was a mass in the cecum area of 65×58 mm (Image 1).
The laboratory findings of the patient were RBC: 3.63×106, PLT: 635×103, RDW: 18.4%, MCV: 64.6 fL, MCHC: 28.4 g/dL, MCH: 18.3 pg, Hgb: 6.7 g/dL, Hct: 23.4%, Serum Fe: 11 ug/dL, GGT: 46 IU/L, ALP: 136 IU/L, and Vitamin B12: 186 pg/mL. The results of total urine test showed amber color, slight turbidity, ample bacteria in urine microscopy, and nitrite (+).
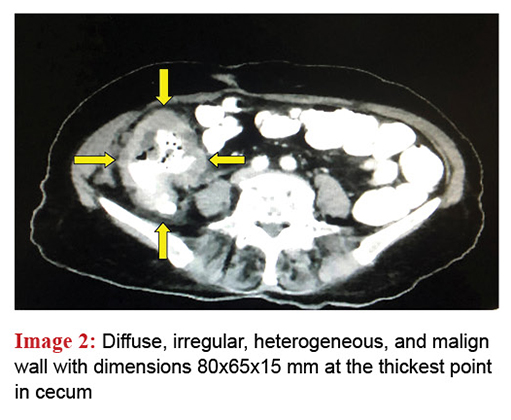
The patient was given treatment for acute cystitis, vitamin B12 deficiency, and iron deficiency. She was referred to general surgery for further examinations and treatment. In the lower abdominal CT, diffuse, irregular, heterogeneous, and malign wall thickening reaching up to 1.5 cm was observed in cecum. Wall thickening was also observed at the joint of terminal ileum and cecum. Contamination and millimetric lymph nodes were observed at the adjacent fat planes (Image 2).
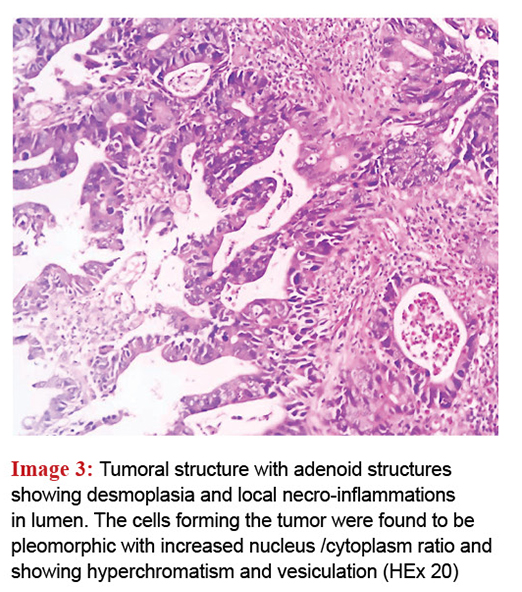
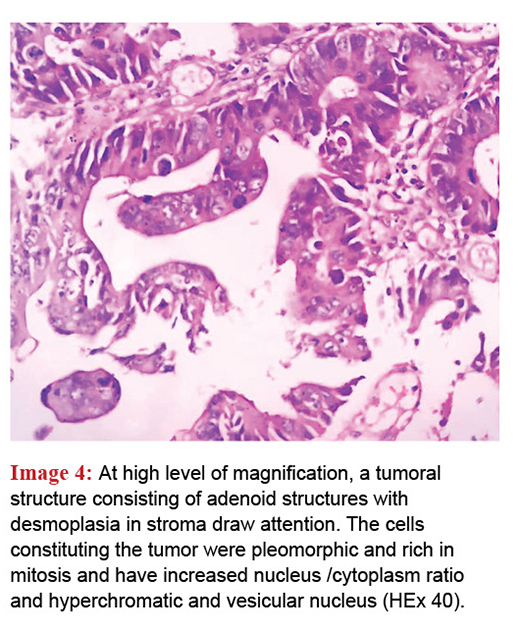
Then, a colonoscopy was planned for the patient but it couldn’t be performed due the insufficient cleaning. Preoperative neoadjuvant radiotherapy was given in order to decrease the tumor size and then the patient underwent surgical operation. Undergone right hemicolectomy, the pathologic analysis of the patient showed that the tumor size was 9x7x1 cm, that tumor reached the serosa, that there was perineural invasion, and that there were 2 metastatic lymph nodes. The diagnosis was reported as adenocarcinoma pT4a, N1a, Mx (Image 3-4).
In mutation analysis performed for the postoperative treatment planning, a BRAF V600E/E2/D mutation was detected. The patient receiving postoperative chemotherapy is in remission and being followed. Patient consent form was received.
Discussion
Although its prevalence at a young age showed an increase in recent years, 90% of colorectal cancers are observed at the ages older than 50 years. Adenocarcinoma cases constitute the largest portion of colorectal cancers.(4,5) Since colorectal cancers develop slowly, the symptoms are observed generally at the advanced level.(4) The symptoms of cecum cancer are detected at the advanced level. These symptoms include anemia, melena, gas – bloating (at the McBurney point seen in appendicitis), nausea, vomiting, and weight loss (losing 5% or more of body weight in 6-12 months).(6) Our patient had loss of appetite and stomachache in lower right quadrant at first. The severe loss of weight (approx. 15 kg) was observed within 3 months. Significant iron deficiency anemia was detected in laboratory analyses.
Standing direct abdominal radiograph, colonoscopy, ultrasonography, barium radiography, and computed tomography can be used for the diagnosis of cecum cancer.(6,7) After the first diagnosis of our patient, the bulk was detected using ultrasonography in our family healthcare center. Tumor size and invasion were found using the abdominal CT.
Significant changes occurred in the colorectal cancer treatment in recent years. As a result of these changes, the rate of mortality significantly decreased. The treatment options include endoscopic and surgical local excision, surgery, neoadjuvant radiotherapy, systemic radiotherapy, extended surgical and local ablative therapies in local and metastatic cases, chemotherapy, immunotherapy, and targeted treatment.(5,8) In the present case, preoperative neo-adjuvant radiotherapy was given in order to shrink the tumor and degrade the grade. Following the radiotherapy, the hemicolectomy was performed.
In colorectal cancer, various genetic and epigenetic changes and risk factors play a significant role in diagnosis, prognosis, molecular targeted treatments, and response to treatment.(9) Various molecules can be used to determine the response to colorectal cancer treatment. BRAF gene plays a role in intracellular signaling and controls the cell division via KRAS.
The mutations in this gene cause uncontrolled cell proliferation. Somatic BRAF gene mutations (V600A, V600D, V600E, and V600KRM) can be observed in malign melanoma, papillary thyroid cancer, and colorectal cancers. The most frequently seen mutation is V600E. Although the patients having this mutation have more aggressive clinical course, the codon of mutation is very important.(9) BRAF gene mutation is observed in 5-10% of stage 4 cancers.(10) BRAF V600E/E2/D mutation was found in the genetic analysis of the present case. Since it was stage 4, the prognosis expectation is at a lower level.
Conclusion
The family medicine discipline has fundamental principles of being the first point of contact with medical system, to offer persons an individualized approach, and to become involved at the early phases of disease development. Based on these characteristics, the present case was diagnosed accurately and she was provided with the guidance necessary for her treatment her treatment.
Conflict of interest:
No potential conflict of interest relevant to this article was reported.
Source of Funding
None declared.
Referanslar
- WHO Coronavirus (COVID-19) Dashboard. Accessed from https://covid19.who.int/ , on 10/12/2021.
- TÜİK Ölüm Nedeni İstatistikleri, 2018. https://data.tuik.gov.tr/Bulten/Index?p=Olum-Nedeni-Istatistikleri-2018-30626 adresinden 30/01/2021 tarihinde erişilmiştir.
- Kolorektal kanser. http://dromersenturk.com/down/kolorektal-kanser.pdf adresinden 31/01/2021 tarihinde erişilmiştir.
- Sav Aydınlı M. Kolorektal Kanser Tanısı Alan Hastaların Koruyucu Hekimlik Açısından Durumu ve Tanı Sürecinin Değerlendirilmesi. Uzmanlık tezi. Ankara Üniversitesi Tıp Fakültesi, Aile Hekimliği Anabilim Dalı, 2011.
- Haraldsdottir S, Einarsdottir HM, Smaradottir A, Gunnlaugsson A, Halfdanarson TR. Krabbamein í ristli og endaþarmi [Colorectal cancer – review]. Laeknabladid 2014 Feb;100(2):75-82.
- Wilkinson J. What is cecum cancer? Signs and Symptoms, Diagnosis, and Treatment. Accessed from https://www.verywellhealth.com/cecum-cancer-796799 on 31/01/2021.
- Nishihara R, Wu K, Lochhead P, Morikawa T, Liao X, Qian ZR, et al. Long-term colorectal-cancer incidence and mortality after lower endoscopy. N Engl J Med 2013; 369: 1095-105.
- Cohen R, Cervera P, Svrcek M, Pellat A, Dreyer C, de Gramont A, et al. BRAF-Mutated Colorectal Cancer: What Is the Optimal Strategy for Treatment? Curr Treat Options Oncol 2017 Feb;18(2):9.
- Canbay E, Buğra D. Kolorektal kanser: Genetik ve moleküler biyoloji araştırmaları hasta tedavisine yeterince yansıyor mu? Ulusal Cerrahi Dergisi 2011; 27(4): 198-205.
- Maughan TS, Adams RA, Smith CG, Meade AM, Seymour MT, Wilson RH, et al. MRC COIN Trial Investigators. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 2011 Jun;18:377(9783):2103-14.


